|
© Borgis - Postępy Nauk Medycznych 7, s. 531-538
Krzysztof Paśnik1, Mariusz Wyleżoł2, *Edward Stanowski1
Surgical treatment of morbid obesity
Metody chirurgicznego leczenia otyłości
1Department of General, Oncological and Thoracic Surgery, Military Institute of Medicine, Warsaw, Poland
Head of Department: Krzysztof Pa?nik, MD, PhD 2Department of Surgery, Military Institute of Aviation Medicine, Warsaw, Poland Head of Department: Mariusz Wyleżoł, MD, PhD Streszczenie
The decision whether a bariatric procedure is to be open or laparoscopic is based on the surgeon´s skill, the patient´s preferences, and the equipment available. Which type of bariatric procedure should be suggested to a patient depends on many factors, which must be thoroughly analyzed and discussed with the patient before the final choice is made. While the decision about the operation is being made, the following factors must be considered: patient´s body mass, comorbidities, dietary habits, patient´s general condition; but also equipment available and surgeon´s skills and experience. In people with high body weight and comorbidities, the surgical treatment should be divided into two stages. In the first one, a simplest procedure aims at achieving the patient´s body mass reduction. The second one – more extended – is to bring a permanent result. The mode of operation depends on patient´s body mass, general condition and comorbidities; operator´s experience in performing different bariatric surgical procedures. At present, surgeons have at their disposal a large range of procedures for obesity treatment. The decision which type and method of bariatric surgery is to be chosen depends on surgeon´s experience, patient´s condition and habits. It should balance between the smallest risk of complications and the biggest body mass reduction. It is not always possible to achieve in a one-stage procedure. In patients with BMI exceeding 50, but also below this value, with comorbidities constituting a significant risk, the surgical treatment should be performed in two stages. The aim is to achieve the patient´s body mass reduction and subsidence of morbidities concomitant with obesity with the smallest risk for the patient by adjusting the surgical treatment modality to surgeon´s experience, patient´s general condition, dietary habits and highest body mass. Such an approach will result in better outcomes and fewer revisional procedures. Słowa kluczowe: classical and laparoscopic surgery, different bariatric surgical procedures
Summary
Na wybór sposobu operacji techniką otwartą czy laparoskopową mają wpływ umiejętności chirurga, preferencje chorego, wyposażenie w odpowiedni sprzęt. Natomiast to, jaki rodzaj operacji bariatrycznej należy zaproponować choremu zależy od wielu czynników, które należy dokładnie przeanalizować i omówić z chorym przed podjęciem decyzji o jego wyborze. Decydując o wyborze operacji należy uwzględnić takie czynniki jak: masa ciała chorego, choroby współistniejące, nawyki żywieniowe, stan ogólny chorego, a także wyposażenie oddziału i umiejętności oraz doświadczenie chirurga. U osób z dużą masą ciała i chorobami towarzyszącymi leczenie operacyjne należy rozłożyć na 2 etapy. W pierwszym należy wykonać operację najprostszą, by po redukcji masy ciała wykonać operację bardziej rozległą, która przyniesie trwały efekt. O sposobie operacji decydują: masa ciała chorego, stan ogólny i choroby towarzyszące, nawyki żywieniowe chorego, doświadczenie operatora w wykonywaniu różnych typów operacji bariatrycznych. Obecnie chirurg ma do dyspozycji całą gamę operacji w chirurgicznym leczeniu otyłości. Od jego doświadczenia i od stanu chorego, jego indywidualnych zachowań zależy wybór sposobu operacji bariatrycznych. Powinna być tak dobrana, aby ryzyko operacji było jak najmniejsze, a redukcja masy ciała jak największa. Nie zawsze jest to możliwe do osiągnięcia w jednym etapie. U osób z masą ciała powyżej 50 kg, a także i mniejszą, z chorobami towarzyszącymi stanowiące duże ryzyko, leczenie operacyjne należy rozłożyć na etapy. Od doświadczenia chirurga, stanu ogólnego chorego, jego nawyków żywieniowych i najwyższej masy ciała należy dobrać sposób leczenia operacyjnego, aby uzyskać redukcję masy ciała, ustąpienie chorób towarzyszących otyłości przy najmniejszym ryzyku dla chorego. Takie postępowanie wpłynie na poprawę wyników leczenia, zmniejszenie liczby operacji rewizyjnych. Key words: chirurgia klasyczna i laparoskopowa, rózne rodzaje operacji bariatrycznych
Methods of surgical obesity treatment can be divided into four groups:
1. Restrictive surgery,
2. A combination of restriction and malabsorption surgery,
3. Malabsorption surgery,
4. Others.
At present, two surgical techniques are used: the open method, called classical – where the surgery is performed through a middle line; and the laparoscopic method using 46 trocars.
Laparotomy surgery technique
The patient lies on the operating table in a supine position with the lower extremities abducted. In order to stabilize the patient on the table, so that the patient will not move when the position of the table changes, the patient is placed on a special mattress and additionally immobilized with wide bands to the stable elements of the table. Once the mattress is deflated, it adjusts to the outline of the patient´s body. This prevents the patient from repositioning during the operation, as well as bed sore formation, and decreases the risk for rhabdomyolysis. It is helpful to tilt the table in such a way that the patient´s head is elevated and the lower extremities lowered (Fowler´s position) or conversely (Trendelenburg position) or to rotate the table sideways. It helps to expose the site operated. In order to decrease the risk for infection, a steridrope should be applied onto the abdominal integument. The passive electrode for electrocoagulation, ultrasound scissors or bipolar vessel sealing system should be placed in a position where it can adhere to the skin well without exerting pressure on tissue. A 34-36 Fr stomach tube is introduced transorally into the patient´s stomach. Diuresis can be monitored through a catheter in the urinary bladder. The incision goes along the midline epigastrically and intra-abdominally. Once the peritoneal cavity is open, it is possible to assess the organs in the abdominal cavity and go on to perform the surgery.
Laparoscopic surgery
The patient is positioned and immobilized in the same way as in the classical surgery. Trocars (4-6) should be placed in such a way that manipulating the instruments should be easy and the operation field clearly visible in the region of the stomach and intestines (upper and middle parts of the abdomen). Most procedures for surgical obesity treatment nowadays are performed laparoscopically. The operator can decide where to place trocars depending on the patient´s body build and mass. In a paper to follow, we will present the equipment used most commonly during surgical obesity treatment procedures.
In the present paper, we describe the most common types of surgery, and the reference list has been presented separately for each type of surgery. Methods which are used relatively rarely have not been included.
Restrictive surgery
Restrictive surgery aims at limiting the capacity of the stomach to take the amount of food eaten. The concept is to divide the stomach with mechanical sutures or banding into two parts: upper (20-50 ml) and lower (the remaining part of the stomach). The anatomical continuity of the alimentary tract is preserved in restrictive surgery. This type of surgery can be performed both laparoscopically and classically.
There exist the following types of restrictive surgery:
1. Vertical Banded Gastroplasty – VBG
2. Laparoscopic performance of vertical banded gastroplasty with MacLean modification
3. Silastic Ring Vertical Gastroplasty – SRVG
4. Adjustable Gastric Banding – AGB
5. Nonadjustable Gastric Banding – NAGB
6. Sleeve Gastrectomy – SG
Vertical Banded Gastroplasty – VBG
When we reach the stomach in the region of the oesophagogastric angle, we incise into the gastrophrenic ligament. In the following stage, we cut the membranous part of the gastrohepatic ligament. Extragastrically, we insert a drain (e.g. Foley catheter), which will be useful during placing a linear stapler. We measure the distance of 6 cm from the oesophagogastric angle distally parallelly to the lesser curvature of the stomach and here, somewhat based on the stomach tube along the lesser curvature of the stomach, using a circular stapler (21-25 mm diameter), we make an opening in both walls of the stomach, stapling them simultaneously. Through the opening, a drain is inserted which goes now along the posterior wall of the stomach from the His angle to the opening. An arm of a mechanical linear stapler with four rows of staples is inserted through the opening. The end of the stapler arm is near the oesophagogastric angle (a 60 mm long magazine). The stapling through the stomach goes parallelly to the lesser curvature, along the stomach tube in the organ. A band is placed onto the part of the stomach that has not been stapled through. The band is made of an inextensible material (prolene, Gore-Tex, Dacron) 7 cm long and 1.5 cm wide, and is placed through the opening which had been made with a circular stapler in the stomach. The band goes around a canal along the lesser curvature of the stomach, which connects the upper and lower parts of the organ. The circumference of the band after it has been sutured is 5 cm, and the diameter of the intragastric canal should be around 1.2 cm. The band prevents the canal connecting both parts of the stomach from stretching. The function can be performed by a band or an elastic silicon drain. Then the procedure is called silastic ring vertical gastroplasty. Before the stomach tube is removed, the alimentary tract tightness should be checked after anatomical changes were made (to attain this, 50-100 ml of either air or aqueous solution of methylene blue is applied with a syringe through the tube). The surgery diagram is presented in figure 1.
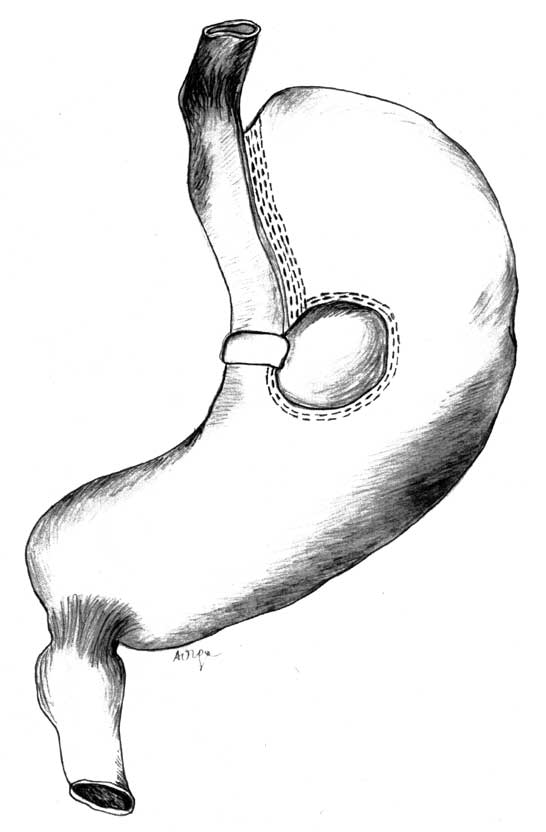 Fig. 1. Scheme of the vertical banded gastroplasty – VBG.
At present VBG surgery is performed with the MacLean modification. The modification is based on the concept of using a linear stapler which can both cut and suture, with which the vertical line of stomach division is cut. This method is universally used in laparoscopic procedures. A diagram of the operation is presented in figure 2.
 Fig. 2. Scheme of the laparoscopic performance of vertical banded gastroplasty with Mac Lean modification – LVBG.
The use of an adjustable silicon band securing the canal between the two parts of the stomach has been described too.
Silastic Ring Vertical Gastroplasty – SRVG
When the peritoneal cavity has been opened in the region of the oesophagogastric angle, we incise into the gastrophrenic ligament and bluntly insert the forefinger towards the lesser curvature. At the lesser curvature, 6 cm from the cardia, we make an opening in the gastrohepatic ligament in the direct vicinity of the stomach wall. A drain (e.g. Foley catheter) is inserted through the opening and leaves the stomach in the region of the oesophagogastric angle. Then, from the side of the lesser curvature we place the arm of a special construction stapler (TA90BN) with four rows of staples. The end of the staple arm is inserted in the region of the oesophagogastric angle. A fragment of the lesser curvature with the gastric tube is placed in a special staple-free „window” of the stapler. The stomach is sutured through and, thus, an upper pouch of 30-50 ml is made. From the side of the lesser curvature (not sutured through) a silicon ring (or band) is applied (like in VBG surgery), which is single sutured to the stomach wall and extends beyond the staple line. At present, this surgery is not performed frequently. Its diagram is presented in figure 3.
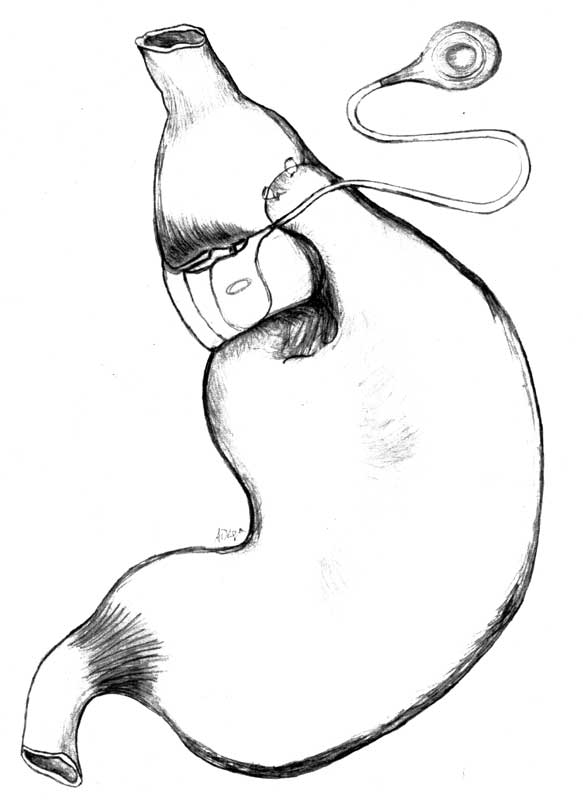 Fig. 3. Scheme of the adjustable gastric bandig – AGB.
Adjustable Gastric Banding – AGB
The concept of this operation, just like the operations of suturing through the stomach, is based on dividing the stomach into an upper part of 15-50 ml volume and the remaining, lower part. To attain this purpose, a band is placed around the stomach, which is connected with a subcutaneous port via a drain. Using a special needle, through the subcutaneous port it is possible to fill in or empty the system, thus deciding about the degree of the restriction – we can regulate the restriction degree.
It is a laparoscopic surgical procedure. When surgical intraperitoneal emphysema of 15-mmHg pressure has been created, the operator inserts trocars into the patient´s peritoneal cavity. The size and number of trocars depends on the patient´s body build.
After introducing a camera into the peritoneal cavity and assessing the other organs in the abdomen, we move aside the left hepatic lobe. Using a cutting-coagulating device, we cut the gastrophrenic ligament, thus unveiling the left crus of the diaphragm. Then we incise the membranous part of the gastrohepatic ligament. Having unveiled the right crus of the diaphragm, we incise the peritoneum over it and make a tunnel, which goes behind the posterior wall of the stomach towards the His angle. An instrument that is helpful in dragging the „goldfinger” band is inserted into the tunnel. Avoiding any damage to the posterior walls of the stomach and oesophagus is mandatory. After checking the system for its tightness, we introduce the band into the abdomen through a trocar of appropriate diameter or directly through the abdominal integument. Then we drag the band through the extragastric tunnel, being aware that the band should be positioned correctly, i.e. the adjustable part should adhere to the stomach wall. The band is fastened with a clip. To prevent the band from slipping off, we suture with non-absorbable sutures above the band the anterior wall of the lower part of the stomach to the upper one. A connector goes from the abdomen through the hole where the trocar was placed to a port, which is placed subcutaneously at the level of the sternum lower part, costal arch or abdominal straight muscle fascia. A valve is fastened to the fascia with non-absorbable sutures. This operation is most often performed laparoscopically, but following similar guidelines, it can be done as an open operation. Figure 3 shows its diagram.
Nonadjustable Gastric Banding – NAGB
The procedure is similar to that of AGB. The band does not have a connecting drain and port. The material used as a band should not be elastic and should be of a defined length, so that once it is applied onto the stomach and both its ends are sewn together, the diameter of the tunnel between the upper and lower stomach pouches should not exceed 1.5 cm.
There are several methods of applying the band onto the stomach. The band goes extragastrically through the membranous part of the gastrohepatic ligament, similarly to the adjustable band encircling the fatty tissue from the side of the lesser curvature. This method is believed to decrease the risk for the band to migrate into the stomach lumen. Another method is letting the band go directly along the stomach wall, along a tunnel made at the level between the first and second vessels on the lesser curvature, below the cardia. The third method, mixed, takes the first stage from the first method and then the band goes along the stomach wall, just like in the second method. The nonadjustable band is rarely used now, although it still has its proponents. The disadvantage of the nonadjustable band is the fact that it is impossible to change the diameter of the canal between the two parts of the stomach; the band is also more likely to migrate into the stomach lumen. The advantages are the low cost and no port-related complications. Some surgeons, while putting on any type of the band, push a balloon-tipped gastric bougie into the stomach in order to calibrate the upper pouch. Inflating the balloon with an adequate amount of fluid (15-50 ml) defines the capacity of the pouch. Figure 4 shows its diagram.
 Fig. 4. Scheme of the nonadjustable gastric banding – NAGB.
Sleeve Gastrectomy – SG
After emphysema is created and trocars inserted (their localization is presented in figure 1), a liver retractor, a grasper and a device to cut and coagulate tissue are introduced into the peritoneal cavity. The stomach preparation is begun from establishing the point that is about 6 cm from the pylorus on the greater curvature of the stomach. Going along the greater curvature, we cut the gastrocolic ligament, gastrosplenic ligament and gastrophrenic ligament until the His angle. We insert into the stomach a gastric tube, usually of 36 Fr, and cut the organ with endostaplers. We typically use green, blue or golden magazines (of appropriate staple length and different magazine length from 30 to 60 mm) depending on the stomach wall thickness and the patient´s anatomy. The stomach left becomes sleeve-like from the side of the lesser curvature. In order to achieve a better haemostasis and tightness, stapled lines are covered with absorbable suturing or tissue glue. The excised part of the stomach is removed from the peritoneal cavity through a slightly extended hole where a 12 mm trocar has been. To protect the integument against infection, the removed part of the stomach can be put into a special container. Sleeve gastrectomy is considered anatomically a restrictive procedure. Of note is the fact that the published study findings point to the neurohormonal impact of this surgery on limited food intake. As the result of decreased serum ghrelin levels and increased PYY neurohormone levels, patients after this operation develop anorexia. Figure 5 presents a diagram of SG surgery.
Fig. 5. Scheme of the sleeve gastrectomy SG.
combination of restriction and malabsorption surgery
These procedures limit the possibility of taking in food via stomach division or resection (the restrictive element) and limit food digestion and absorption via shortening the passage of chime in the small intestine (the malabsorption element). These procedures can be performed both classically and laparoscopically.
The most essential surgical procedures combining restriction with malabsorption include:
Biliopancreatic diversion – duodenal switch – BPD-DS
Roux-en-Y gastric bypass – RYGB
The restriction-malabsorption surgery procedures are difficult to perform, need a very skilful operator both in open and laparoscopic surgery, and are associated with a higher risk for complications. Patients qualified for this type of surgery have BMI> 40 and like sweets. The procedures require at least two anastomoses to be made (gastroenterostomy and enteroenterostomy, and cross-sectional closing of the stomach and/or intestine). The advantages are the biggest and most permanent body weight loss and high quality of life. The differences between the types of surgery described above refer to differences in the pouch size made from stomach and different lengths of the alimentary, enzymatic and digestive loops. A diagram of restrictive surgery is presented in figure 6, and the characteristics of individual elements (the sizes of stomach, enzymatic, alimentary and common loops) are given in table 1.
Table 1. The lenght and volume of the components in restrictive procedures.
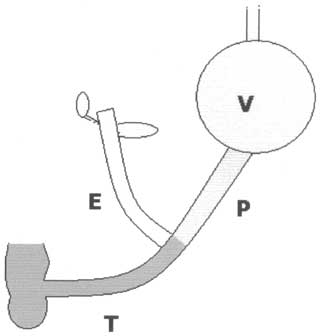 Fig. 6. The scheme of basic restrictive techniques:
V – the part of the stomach participating in food passage, E – biliopancreatic limb, P – alimentary limb, T – common limb. Biliopancreatic diversion – duodenal switch – BPD-DS
In the first stage of the operation, we perform a sleeve resection of the stomach (the technique is described above). We cut the duodenal bulb 5 cm below the pylorus. The small intestine is divided at 250 cm from the ileocolic valve. The distal loop of the small intestine is anastomosed with the duodenal bulb. The proximal loop of the incised small intestine is sutured into the distal loop at 100 cm from the ileocolic valve. In this way, an alimentary loop (150 cm long) and a common digestive loop (100 cm long) are created. The remaining part of the intestine is an enzymatic loop. Duodenoenterostomy can be stapled or made manually, both as end-to-end anastomosis and end-to-side anastomosis. Enteroenterostomy in classical surgery is typically made manually as end-to-side anastomosis. In laparoscopy, it is usually stapled end-to-side anastomosis. A diagram of the procedure is presented in figure 7.
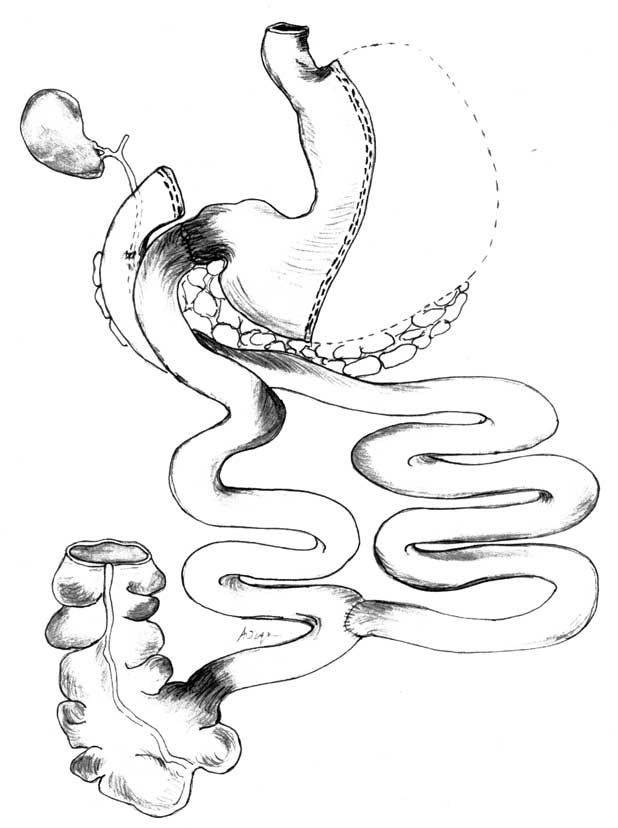 Fig. 7. Scheme of the biliopancreatic diversion – duodenal switch – BPD – DS.
Roux-en-Y Gastric Bypass – RYGB
It is much easier to perform a laparoscopic procedure if modern electrosurgery tools or an ultrasound knife are used. The procedure is begun by cutting the stomach and making a 30 ml upper pouch. The staple line usually goes between the first and second branch of the left gastric artery and the His angle. A cutting-and-suture stapler is used. In the classical technique, it is usually a single application; in laparoscopy, multiple endostaplers are applied. The upper part of the stomach often needs to be „stripped” of the surrounding fatty tissue. The small intestine is divided at 70-100 cm from the suspensory ligament. The distal loop of the small intestine is anastomosed with the upper pouch of the stomach. The proximal loop of the incised small intestine is sutured into the distal loop at 100-150 cm from the gastroenterostomy. Thus, we obtain an alimentary loop (100-150 cm long) and an enzymatic loop (70-100 cm long). The remaining part of the intestine makes a digestive loop. Gastroenterostomy can be made manually side-to-side. A linear stapler or a circular one can be used too. When a circular stapler is used, the anvil is typically inserted transorally on a tube and the stapler through the abdominal wall, after removing a trocar, beneath the left costal arch. The anastomosis is performed with the „end insertion technique”. When the gastroenterostomy is made, the end of the intestine is closed with another linear stapler. There is a variant of the gastric bypass procedure where the alimentary loop is longer and, consequently, the digestive loop shorter. It is long limb Roux-en-Y gastric bypass (LLRYGB). In the case of distal Roux-en-Y gastric bypass (DRYGB), the enzymatic loop is sutured into the alimentary loop at 100 cm from the ileocolic valve. Some surgeons additionally use a silicon drain or synthetic ribbon to fasten around the stomach above the gastroenterostomy. A diagram of this gastric bypass is presented in figure 8.
 Fig. 8. Scheme of the Roux – en – Y gastric by – pass RYGB.
Malabsorption surgery
Biliopancreatic diversion – BPD
A subcardial 250 ml pouch is made by resecting the remaining part of the stomach. Linear staplers are used to create the pouch from the upper part of the stomach and to close the duodenal stump. The small intestine is divided at 250 cm from the ileocolic valve. The proximal loop of the incised small intestine is sutured into the distal loop at 50 cm from the ileocolic valve. In this way, we obtain an alimentary loop (200 cm long) and a digestive loop (50 cm long). The remaining part of the intestine makes an enzymatic loop. Gastroenterostomy can be stapled and performed manually. In the classical surgery, enteroenterostomy is typically made manually end-to-side. In laparoscopy, it is stapled side-to-side. There is a BPD variant, where the subcardial pouch size and intestinal loop length are adjusted to the patient´s dietary habits and baseline body mass. It is called ad hoc stomach ad hoc alimentary limb (AHS-AHAL) BPD. In still another, the Roux loop is made at mid-length of the small intestine – it is called half to half BPD. A diagram of BPD surgery is presented in figure 9.
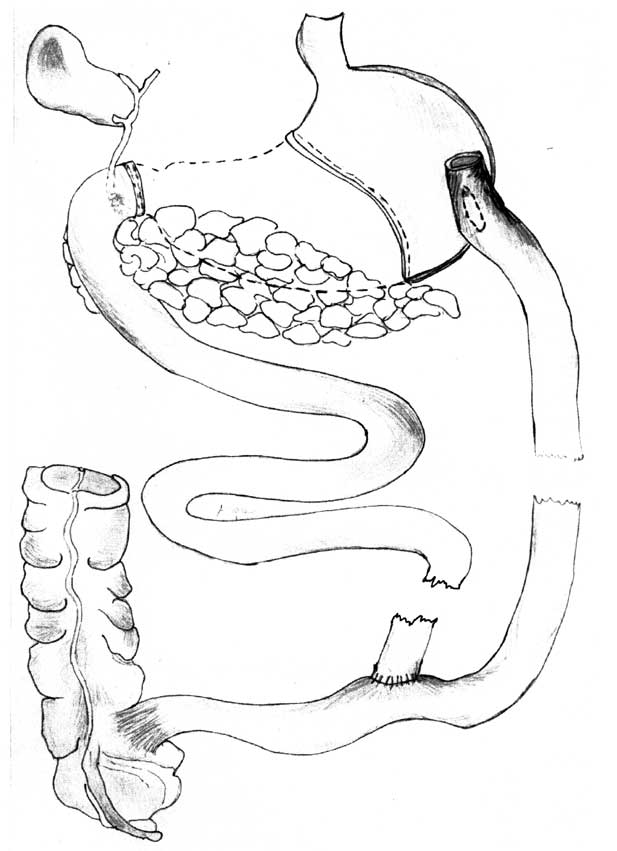 Fig. 9. Scheme of the biliopancreatic diversion – BPD.
Much more severe intra and post surgical complications can be expected in morbidly obese patients with comorbidities such as hypertension, diabetes mellitus and metabolic syndrome. In such patients treatment of obesity should be divided into stages. The first stage covers a conservative treatment, a dietary regimen, pharmacotherapy, kinesitherapy and a provisional insertion of the stomach balloon. Having achieved even a small improvement in terms of a patient´s general condition and body mass loss the next step can be made – a surgery. It should be the simplest, the shortest and carrying the least possible complications. The second stage includes different surgical techniques such as insertion of the adjustable gastric band, sleeve gastrectomy and vertical banded gastroplasty. When a significant body weight reduction is achieved with no tendency to regain weight the operational treatment can be terminated. If a body weight increases after surgery ("the yoyo effect”) the next stage is necessary.
The third stage covers more complicated and complex procedures (e.i. with two anastomoses), such as gastric bypass, biliopancreatic diversion (BPD), biliopancreatic diversion – duodenal switch (BPD-DS), mini gastric by-pass (tab. 2).
Table 2. Shows the stages of operative treatment for morbid obesity.
This way of treatment reduces the risk of intra and postoperative complications, provides good results in keeping lower body weight, improves or eliminates comorbidities. The choice of a surgical technique in every stage of treatment depends largely on a patient´s condition and a surgeon´s experience.
The surgical methods presented above can be performed both in the classical way and laparoscopically. Such a large variety of surgical methods and techniques enables a surgeon to choose an individual mode of operating for each patient depending on indications of the patient´s condition.
The diagrams depicting particular operation stages were made by Ms Agnieszka Ozga, MA – thank you very much.
Piśmiennictwo
1. Mason EE: Vertical banded gastroplasty for obesity. Arch Surg 1982; 117: 701-6.
2. MacLean LD, Rhode BM, Forse RA: A gastroplasty that avoids stapling in continuity. Surgery 1993; 113: 380-8.
3. Paśnik K, Krupa J, Stanowski E: Vertical banded gastroplasty: 6 years experience at a center in Poland. Obes Surg 2005; 15: 223-7.
4. Wylezol M, Pardela M, Gluck M: Outcome of vertical banded gastroplasty procedures conducted in Poland in 1993-1999 according to Bariatric Analyzing and Reporting Outcome System (BAROS). Obes Surg 2000; 10: 321.
5. Wang W et al.: Laparoscopic vertical banded gastroplasty: 5-year results. Obes Surg 2005; 15: 1299-303.
6. Laws H: Standardized gastroplasty orifice. Am J Surg 1981; 141: 393-4.
7. Alper D, Ramadan E, Vishne T: Silastic ring vertical gastroplasty – long-term results and complications. Obes Surg 2000; 10: 250-4.
8. Urbain P, Heiderich B: Six years´ experience with minilaparotomy silastic ring vertical gastroplasty. Obes Surg 2001; 11: 258-64.
9. Wolf A, Kortner B, Kuhlman HW: Silastic Ring Vertical Gastroplasty Using a Modified TA 90 BN. Obes Surg 1996; 6: 254-7.
10. Kuzmak L: A review of seven years´ experience with silicon gastric banding. Obes Surg 1991; 1:403-8.
11. Wyleżoł M, Pardela M, Gluck M: Swedish adjustable gastric band/AGB/implanted laparoscopically in the treatment of morbid obesity – the first experience in Poland. Med Sci Monit 2000; 6: 441-5.
12. Dargent J: Laparoscopic adjustable gastric banding: lessons from the first 500 patients in a single Institution. Obes Surg 1999; 9: 446-52.
13. Favretti F et al.: Laparoscopic adjustable gastric banding in 1,791 consecutive obese patients: 12-year results. Obes Surg 2007; 17: 168-75.
14. Oria HE: Gastric banding for morbid obesity. Eur J Gastroenterol Hepatol 1999; 11: 105-14.
15. Fuks D et al.: Results of laparoscopic sleeve gastrectomy: a prospective study in 135 patients with morbid obesity. Surgery 2009; 145: 106-13.
16. Marceau P et al.: Duodenal switch: long-term results. Obes Surg 2007; 17: 1421-30.
17. Baltasar A, Bou R, Begochea M: Duodenal switch: an effective therapy for morbid obesity – intermediate results. Obes Surg 2001; 11: 54-8.
18. Paśnik K, Kostewicz W: Laparoskopowe leczenie otyłości. Podręcznik. Chirurgia Laparoskopowa pod red. W. Kostewicza PZWL 2002.
19. Brolin RE: Gastric bypass. Surg Clin North Am 2001; 81: 1077-95.
20. De Maria EJ et al.: Results of 281 consecutive total laparoscopic Roux-en-Y gastric bypasses to treat morbid obesity. Ann Surg 2002; 235, 640-7.
21. Nguyen NT, Goldman C, Rosenquist CJ: Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. Ann Surg 2001; 234: 279-89.
22. Capella JF, Capella RF: An assessment of vertical banded gastroplasty – Roux-en-Y gastric bypass for the treatment of morbid obesity. Am J Surg 2002; 183: 117-23.
23. Fobi MA: The surgical technique of the banded Roux-en-Y gastric bypass. J Obes Weight Reg 1989; 8: 99-102.
24. Strzelczyk J: Ocena współczesnych wyników chirurgicznego leczenia otyłości metodą ominięcia żołądka według Masona oraz propozycja własnego sposobu zamknięcia rany z zastosowaniem siatki polipropylenowej. Rozprawa habilitacyjna. Łódź 2003.
25. Pardela M, Wyleżoł M, Gluck M: Laparoskopowe wyłączenie żołądkowe w leczeniu skrajnej otyłości. 60 Jubileuszowy Zjazd Towarzystwa Chirurgów Polskich Warszawa 2001 r. Streszczenie: 921.
26. Scopinaro N, Gianetta E, Adami GF: Biliopancreatic diversion for obesity at eighteen years. Surgery 1996; 119: 261-8.
27. Scopinaro N, Marinari G, Camerini G: Laparoscopic standard biliopancreatic diversion: technique and preliminary results. Obes Surg 2002; 12, 241-4.
28. Wylezol M: Biliopancreatic diversion in Poland. J Physiol Pharmacol 2005; 56 Suppl 6: 117-26.
29. Miller KA: Implantable electrical gastric stimulation to treat morbid obesity in the human: operative technique. Obes Surg 2002; 12, 1: 17-20.
30. Rutledge R: The mini-gastric bypass: experience with the first 1,274 cases. Obes Surg 2001; 11: 276-80.
otrzymano/received: 2009-04-01 zaakceptowano/accepted: 2009-06-03 Adres/address: *Edward Stanowski Department of General, Oncological and Thoracic Surgery, Military Institute of Medicine Szaserów Str. 128, 00-909 Warsaw tel.: (0-22) 681 63 00 e-mail: chirstan@wim.mil.pl Pełna wersja artykułu Surgical treatment of morbid obesity dostępna w Czytelni Medycznej Borgis. |
  Proszę kliknąć w wybraną okładkę aby przejść na stronę czasopisma
 |






Chcesz być na bieżąco? Polub nas na Facebooku: strona Wydawnictwa na Facebooku |