|
© Borgis - Postępy Nauk Medycznych 7, s. 511-513
*Anna Kopińska1, Małgorzata Krawczyk-Kuliś1, Przemysław Pencak2, Joanna Bienias1, Sławomira Kyrcz-Krzemień1
Samoistne krwawienie z przewodu pokarmowego pierwszym objawem zapalenia wyrostka robaczkowego u pacjenta z umiarkowaną postacią hemofilii B
Spontaneous intestinal bleeding as the first manifestation of appendicitis in a patient with moderate hemophilia B
1Department of Hematology and Bone Marrow Transplantation, Silesian Medical University, Katowice
Head of Department: prof. Sławomira Kyrcz-Krzemień, MD, PhD 2Department of Radiology, Mielęcki Public Hospital, Katowice Head of Department: Przemysław Pencak, MD, PhD Streszczenie
Prezentujemy 22-letniego pacjenta z umiarkowaną hemofilią B przyjętego do naszej Kliniki z powodu krwawienia z przewodu pokarmowego z towarzyszącymi dolegliwościami bólowymi w jamie brzusznej. Badanie ultrasonograficzne, jak również tomografia komputerowa potwierdziły zapalenie wyrostka robaczkowego. Przeprowadzono leczenie operacyjne, uzyskując ustąpienie dolegliwości klinicznych. Podczas hospitalizacji pacjent otrzymywał leczenie substytucyjne czynnikiem IX. Według naszej wiedzy jest to pierwszy opis przypadku zapalenia wyrostka robaczkowego objawiającego się samoistnym krwawieniem z przewodu pokarmowego u pacjenta z umiarkowaną postacią hemofilii B. Słowa kluczowe: hemofilia B, zapalenie wyrostka robaczkowego, krwawienie z przewodu pokarmowego
Summary
Herein, we present a 22-year-old patient with moderate hemophilia B admitted to our department for intestinal bleeding and diffuse abdominal pain. Ultrasonography examination and computing tomography were consistent with a diagnosis of appendicitis. The patient improved clinically after surgery. During hospitalization the replacement therapy was given. To our best knowledge this is the first report on spontaneous intestinal bleeding as a first manifestation of appendicitis in a patient with moderate hemophilia. Key words: hemophilia B, appendicitis, intestinal bleeding
Introduction
Hemophilia B is an inherited uncommon X-linked disorder caused by a lowered or absent plasma factor IX. It can be classified as mild, moderate or severe (1). Only one or two out of every one hundred thousand people have this type of hemophilia. In hemophilia B patients spontaneous bleeding occurs in severe cases. Moderately deficient bleeding is associated with trauma or surgery. We present a patient treated in our clinic department for moderate hemophilia B with spontaneous intestinal bleeding as the first syndrome of appendicitis. 20-30 years ago a lot of surgical procedures were contraindicated for people with congenital bleeding disorders (2). Nowadays they could be safely treated also using complicated, invasive methods. Before, during and after an operation the appropriate factor replacement should be maintained (3).
Case description
A 22-year-old male with moderate hemophilia B (factor IX level at diagnosis was 3.5%). There was no history of bleeding. During that time he did not present any other episodes of severe bleeding. The patient had been treated since his childhood with the use of factor IX concentrates. On admission he presented abdominal pain, nausea and bloody diarrhea. Fever was not present.
On physical examination at the admission the abdomen was painful with peritoneal irritation signs. Hematology test were normal. Biochemistry test showed an elevated level of C reactive protein up to 115 mg/l (norm < 5 mg/l). Coagulation test revealed prolonged aPTT (activated partial thromboplastin time) 47 seconds. The analyses presented hemoglobin 15.3 g/dl, WBC 5.5 G/l (with granulocytosis 81%), HCT 44%. After three hours the level of hemoglobin decreased to 12 g% because of bleeding. Ultasonography examination revealed: hepatosplenomegaly. All other abdominal organs were within normal limits. There was no ascites. A mild dilatation of cecum area was observed. Overall condition was getting worse in the next 2 days and symptoms of peritonitis with fever occurred. An abdominal radiography showed intestinal distention with thin air-fluid level in the right part abdomen. CT scan of the abdomen confirmed the diagnosis of appendicitis with signs of periappendicular adipose-tissue inflammation and a pericecal thin liquid layer (fig. 1).
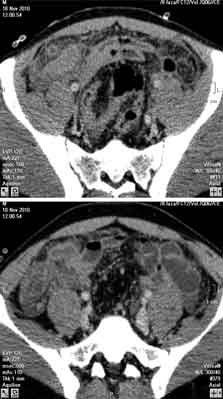 Fig. 1. CT scans with the contrast enhancement, 4 cm caudal to cecum, shows a high attenuation of mesenteric fat and distended small bowel loops also with some fluid (level) and gas collection. Some small amount of interloop fluid collection is seen. The abnormal appendix cannot be definitively identified.
The patient received 6200 IU of factor IX prior to surgery and 6200 IU post surgery with continuous infusion in order to keep the plasma concentration level at 30% for the next 12 days. The intravenous administration of factor IX concentrates (4800 IU) was given every 12 hours in the first day after the operation and once a day (4800 IU) during the next 2 days. Then the dose was slowly decreased. The infusion was well tolerated. There were no other complications. During the surgery the abscesses in the right appendiceal side was found. The histological examination revealed the infiltration of the appendix, the appendix mesentery and the surrounding adipose tissue. The substitution treatment with factor IX was continued. The level of factor IX in patients’ blood during hospitalization was kept on the level of 30%. No hemorrhagic events after surgeon were detected. On the fifth day after the operation the patient was discharged.
Discussion
Spontaneous intestinal bleeding is not a typical manifestation of appendicitis. It may occur in patients with congenital coagulopathy such as severe hemophilia, but it is rare in moderate and mild variant. To our best knowledge it is the first case of non-traumatic bleeding in patient with moderate hemophilia B. It should be understood that spontaneous bleeding could be the earliest manifestation of appendicitis. On admittance the symptoms were not consistent with appendicitis. Patient with hemophilia could manifest untypical symptoms of sharp abdominal diseases. One should remember that the complete diagnostic work-up is therefore delayed. Ultrasonography and computed tomography may fail to identify the disease. Treatment with factor concentrate should be started promptly. One should also remember that treatment patient with congenital coagulopathy should take place in the hospitals with great experience (hemophilia treatment center). The level of factor IX is easy to be monitored in post-surgery bleeding. It should be mentioned that hemophilia patients undergoing surgery should keep safety level of factor IX. In our case pre- and postoperative factor IX level remained > 30%. However there is still lacking recommendation regarding the required level of factor IX before general surgery (3). In orthopedic surgery as well as in laryngology the level is recommended to be above 80% due to higher risk of life-threatening bleeding (4).
In summary, appendicitis and other abdominal diseases should be suspected in cases of non-traumatic and non-iatrogenic bleeding in patients with congenital coagulopathies such as hemophilia. Spontaneous bleeding is not always associated with hemophilia even if the initial work-up fails to indicate coagulopathy as the main causes of bleeding. Piśmiennictwo
1. Rudowski W: Major surgery in hemophilia. Ann R Coll Surg Engl 1981; 65: 111-117.
2. Pool JG, Hershgold EJ, Pappenhagen AR: High potency antihaemophilic factor concentrate prepared from cryoglobulin precipitate. Nature 1964; 203: 312.
3. Aryal K, Wiseman D, Siriwardena AK et al.: General surgery in patients with a bleeding diathesis. How we do it. World J Surg 2011; 35: 2603-2610.
4. Watts RG, Cook RP: Operative management and outcomes in children with congenital bleeding disorders. A retrospective review at a single hemophilia treatment centre. Haemophilia 2012; 18: 421-425.
otrzymano/received: 2013-03-06 zaakceptowano/accepted: 2013-05-08 Adres/address: *Anna Kopińska Department of Hematology and Bone Marrow Transplantation Silesian Medical University ul. Dąbrowskiego 25, 40-037 Katowice tel.: +48 (32) 259-12-00 fax: +48 (32) 255-49-85 e-mail: cauda.equina@wp.pl Artykuł Samoistne krwawienie z przewodu pokarmowego pierwszym objawem zapalenia wyrostka robaczkowego u pacjenta z umiarkowaną postacią hemofilii B w Czytelni Medycznej Borgis. |
  Proszę kliknąć w wybraną okładkę aby przejść na stronę czasopisma
 |






Chcesz być na bieżąco? Polub nas na Facebooku: strona Wydawnictwa na Facebooku |