© Borgis - Medycyna Rodzinna 1, p. 6-10
*Elżbieta Mazur
Atypowe zapalenia płuc – obraz kliniczny, diagnostyka mikrobiologiczna
The atypical pneumonias – clinical symptoms and microbiological diagnosis
Katedra Mikrobiologii Lekarskiej Uniwersytetu Medycznego w Lublinie
Kierownik: prof. dr hab. Maria Kozioł-Montewka
Summary
The study presents state-of-the-art knowledge on the atypical pneumonias. The term "atypical pneumonia” was first applied to clinically milder course of this disease in comparison to typical, pneumococcal pneumonia. Currently atypical pneumonias mean lower respiratory tract infections due to specific, atypical pathogens, different from typical bacteria. They are now considered to be systemic infectious diseases with a pulmonary component and may be differentiated clinically from typical pneumonias by the pattern of extrapulmonary organ involvement which is characteristic for each atypical pneumonia. Although differentiation of pneumonias based on clinical presentation can help in the preliminary diagnosis, it´s not sufficient, since it is now widely recognized that the clinical course of pneumonia may be similar whether caused by typical or atypical respiratory pathogens. The importance of the atypical pneumonias is not related to their frequency but to difficulties in their diagnosis, and their nonresponsiveness to beta-lactam therapy.
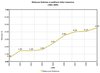
The most frequent etiological agents causing atypical pneumonias were characterized, namely Mycoplasma pneumoniae, Chlamydia (Chlamydophila) pneumoniae and Legionella spp. Clinical symptoms and microbiological diagnosis allowing to differentiate atypical from typical bacterial pneumonias were described. Particular attention was dedicated to infections caused by Legionella spp., since the number of confirmed Legionnairs´ disease cases is considered to be underestimated in comparison with its real prevalence.
Key words: atypical pneumonias, Mycoplasma pneumoniae, Chlamydia ( Chlamydophila) pneumoniae, Legionella spp.
Piśmiennictwo
1. Cunha B.A.: The atypical pneumonias: clinical diagnosis and importance. Clin. Microbiol. Infect., 2006; 12, Suppl. 3: 12-24. 2. Godet C., et al.: Legionnaire´s pneumonia: is there really an interstitial disease? Eur. J. Radiol., 2007; 61: 150-153. 3. Hammerschlag M.R.: Pneumonia due to Chlamydia pneumoniae in children: epidemiology, diagnosis, and treatment. Pediatr. Pulmonol., 2003; 36: 384-390. 4. Mills G.D., et al.: Effectiveness of beta-lactam antibiotics compared with antibiotics active against atypical pathogens in non-severe community acquired pneumonia: meta-analysis. BMJ 2005; doi:10.1136/bmj.38334.591586.82. 5. File T.M., et al.: Guidelines for empiric antimicrobial prescribing in community-acquired pneumonia. Chest, 2004; 125:1888-1901. 6. Blasi F.: Atypical pathogens and respiratory tract infections. Eur. Respir. J., 2004; 24: 171-181. 7. Wolf J., Daley A.J.: Microbiological aspects of bacterial lower respiratory tract illness in children: atypical pathogens. Paediatr. Respir. Rev., 2007; 8: 212-220. 8. Diederen B.M.W.: Legionella spp. and Legionnaires´ disease. J. Infect., 2008; 56: 1-12. 9. Stra°lin K.: Usefulness of aetiological tests for guiding antibiotic therapy in community-acquired pneumonia. Int. J. Antimicrob. Agents 2008; 31: 3-11. 10. Schneeberger P.M., et al.: Diagnosis of atypical pathogens in patients hospitalized with community-acquired respiratory infection. Scand. J. Infect. Dis., 2004; 36, 4: 269-73. 11. Thibodeau K.P., Viera A.J.: Atypical pathogens and challanges in community-acquired pneumonia. Am. Fam. Physician, 2004; 69: 1699-706. 12. Principi N., Esposito S.: Emerging role of Mycoplasma pneumoniae and Chlamydia pneumoniae in paediatric respiratory tract infections. Lancet Infectious Diseases 2001; 1: 334-344. 13. Kumar S., Hammerschlag M.R.: Acute respiratory infection due to Chlamydia pneumoniae: current status of diagnostic methods. Clin. Infect. Dis., 2007; 44: 568-576. 14. van de Garde E., et al.: Prior outpatient antibiotic use as predictor for microbial aetiology of community-acquired pneumonia: hospital-based study. Eur. J. Clin. Pharmacol., 2008; 64: 405-410. 15. Szewczyk E.M.: Diagnostyka mikrobiologiczna, Wydawnictwo Naukowe PWN, 2005. 16. Waites K.B., Talkington D.F.: Mycoplasma pneumoniae and its role as a human pathogen. Clin. Microbiol. Rev., 2004; 17: 697-728. 17. Grayston J.T.: Infections caused by Chlamydia pneumoniae strain TWAR. Clin. Infect. Dis., 1992;15: 757-763. 18. Fields B.S., et al.: Legionella and Legionnaires´ Disease: 25 years of investigation. Clin. Microbiol. Rev., 2002; 15: 506-526. 19. Krogulska B.: Legionella - charakterystyka, zagrożenia zdrowotne, występowanie w środowisku naturalnym i w sztucznych rezerwuarach wody. [W:] Legionella: występowanie, metody wykrywania i identyfikacji oraz uregulowania prawne - konferencja z warsztatami szkoleniowymi. Lublin, 7-9 grudnia 2007. 20. Mrozińska M.: Zapalenie płuc o etiologii Legionella pneumophila u trojga dzieci - opis przypadków. Przegl. Epidemiol., 2005; 59: 851-857. 21. Roig J., Rello J.: Legionnaires´ disease: a rational approach to therapy. JAC 2003; 51: 1119-1129. 22. Stypułkowska-Misiurewicz H., Pancer K.: Legioneloza w Polsce w latach 2001-2002 na tle sytuacji epidemiologicznej w Europie. Przegl. Epidemiol., 2003; 57: 599-606. 23. Stypułkowska-Misiurewicz H., Pancer K.: Legioneloza - nowe zagożenie w Polsce. Przegl. Epidemiol., 2002; 56: 567-76. 24. Weiss K., Tillotson G.S.: The controversy of combination vs monotherapy in the treatment of hospitalized community-acquired pneumonia. Chest 2005; 128: 940-946. 25. Shefet D., et al.: Empirical atypical coverage for inpatients with community acquired pneumonia. Systemic review of randomized controlled trials. Arch. Intern. Med., 2005; 165: 1992-2000.
otrzymano/received: 2007-12-14
zaakceptowano/accepted: 2007-12-27
Adres/address:
*Elżbieta Mazur
Katedra Mikrobiologii Lekarskiej
ul. Chodźki 1, 20-093 Lublin,
tel. 081 742 37 85
e-mail: elamazur@yahoo.com